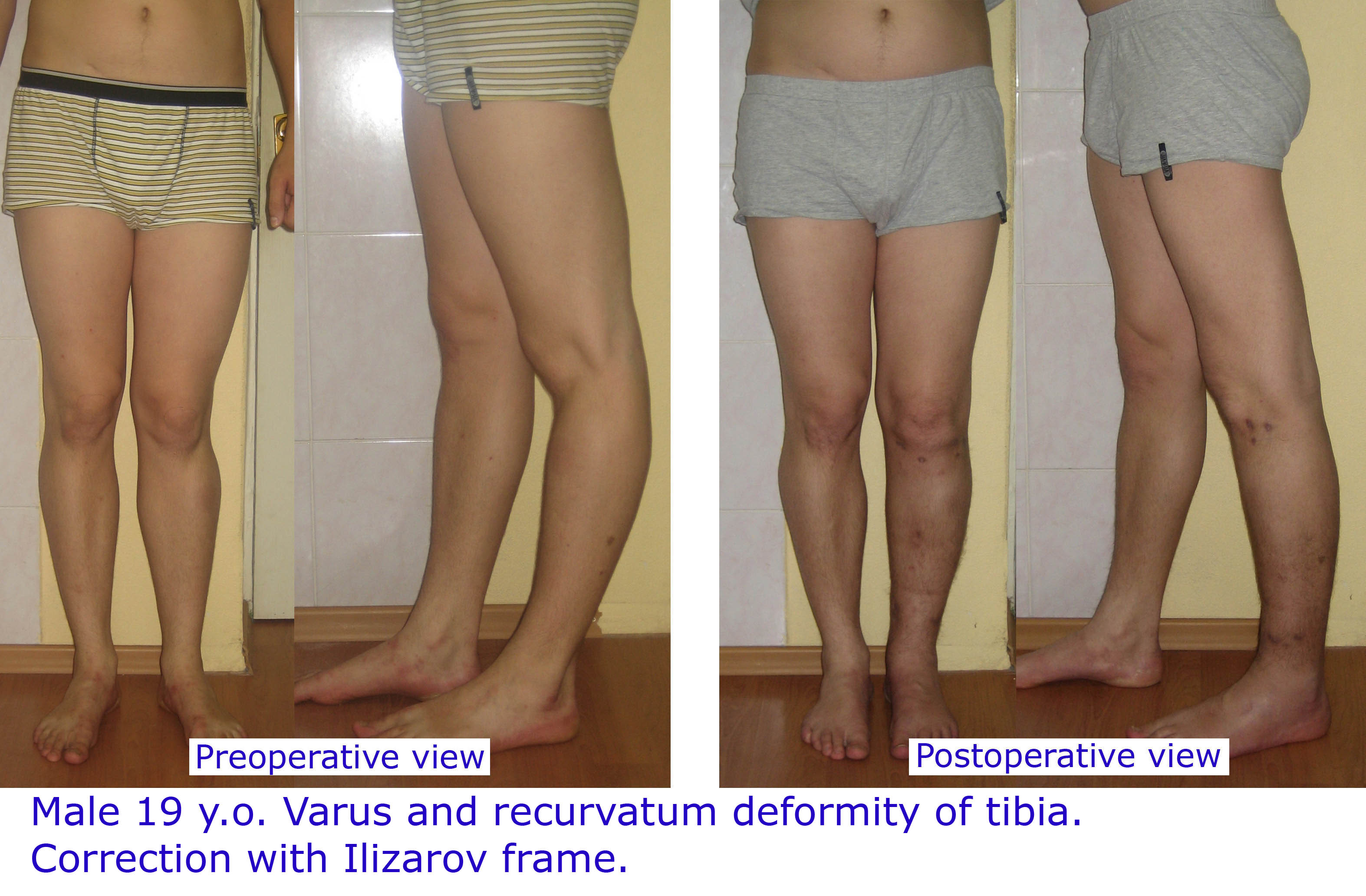
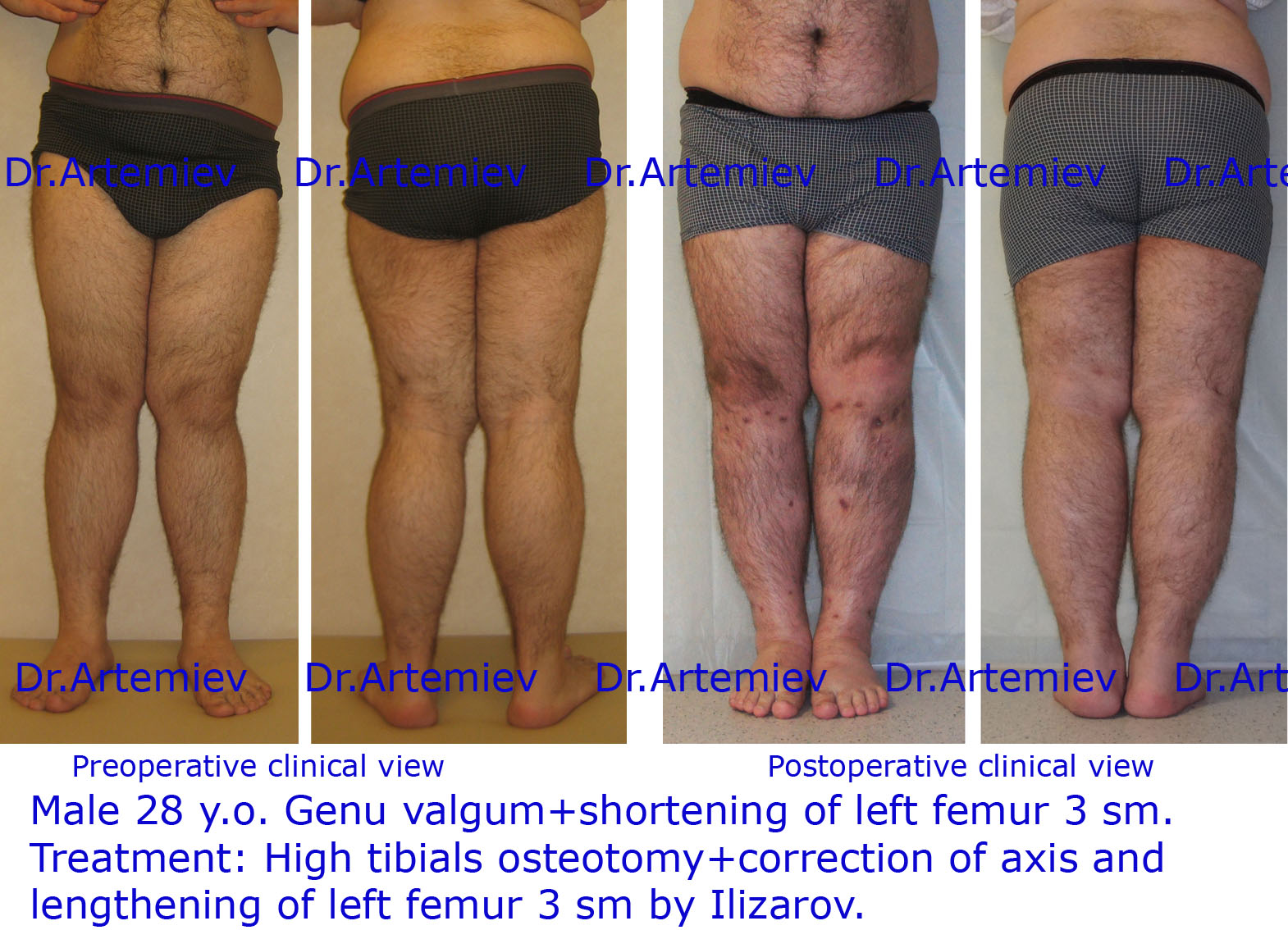
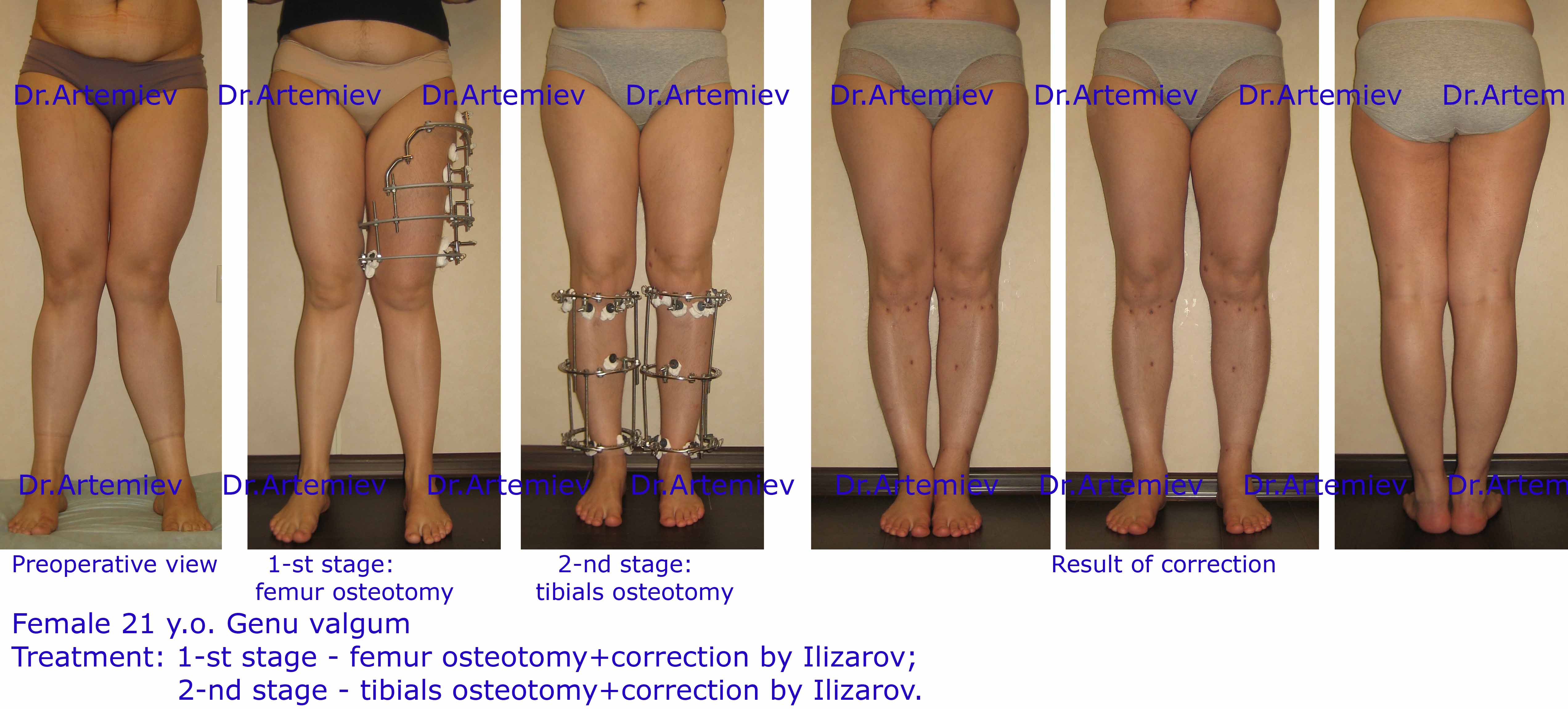
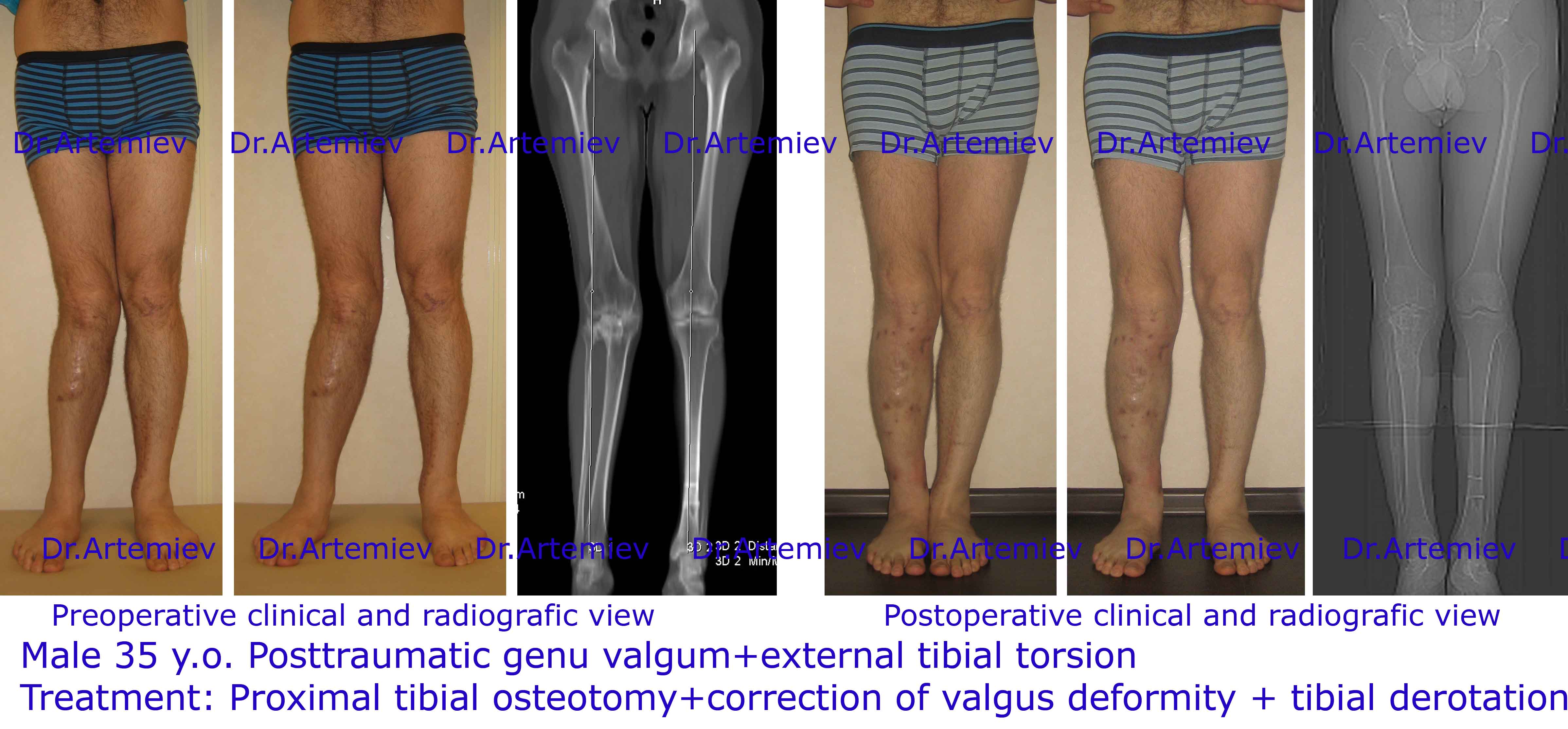
Knock knees (valgus deformity) correction
True X-shape curvature (valgus deformity) is the distance between feet and closed ankles standing up right.
-
 Ideal legs Bow legs False curvature Knock knees
Ideal legs Bow legs False curvature Knock knees
Main causes of genu valgum (knock knees):
- Idiopatic genu valgum;
- Osteoarthritis of the knee;
- Posstraumatic deformity of femur or tibia;
- Diseases.
It's broadly classified into physiological (idiopatic) and pathiological; the latter could be unilateral or bilateral. Genu valgum is often characterized by asymmetric deformity as well as it combination with other types of deformity: knee hyperextension, rotation and legs lengs discrepancy.
Idiopatic genu valgum
Knock knees are more prevalent in residents of Europe and North Amirica however it occurs worldwide.
You can easily define your leg shape according to classification (Dr.Artemie, 2001) by youself abd consider if you need to change somthing or not.
- Ideal legs. Knees, calves and ankles are touching, three intervals between them.
- Bow legs (genu varum, true O-shaped curvature). Knees can't be attached to each other when ankles are touching. The main reason - varus deformity of the tibia below the knee.
- False curvature. It is in unique structure of soft tissues on the shin.
- Knock knees (genu valgum, true X-shaped curvature) - knees are touching, ankles are separate. The main reason - valgus deformity of the femur.
It's very important than modern correction of legs deformity allows not only achieve pleasing cosmetic result but to prevent progress of osteoarthritis of knees in mature and adulthood.
Osteoarthritis of the knee
Knock knees is associated with a reduced quality of life, substantial gait disturbance and can increase the risk of isolated compartment osteoarthritis of the knee. X-ray assesment is essential to pre-operative planning of osteotomies. In case of genu valgum due to deformity of the femoral bone the osteotomy proximal to the knee joint is performed. On the contrary the osteotomy distal to the knee is indicated if tibial deformity is diagnosed.
Surgical correction of tibial bone is less technically demanding and has a lower risk of complications comparing to femoral interventions. Nevertheless in case of significant valgus deformity surgical reconstruction of the most involved segment is required. X-shape deformity correction is basically similar to genu varum ccorrection. Given this main features of operative technique as well as posoperative care are similar in both procedures.
Gallery