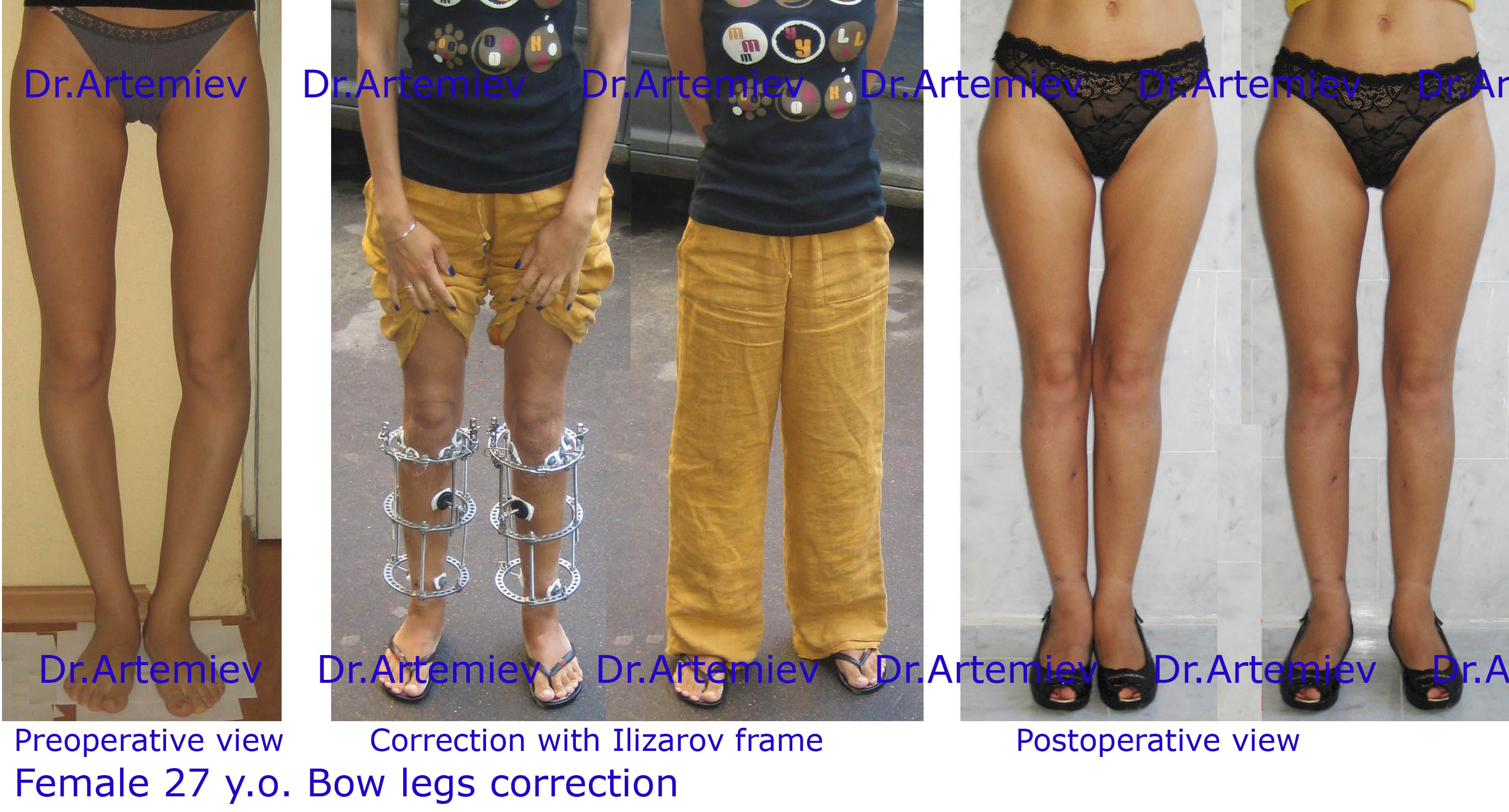
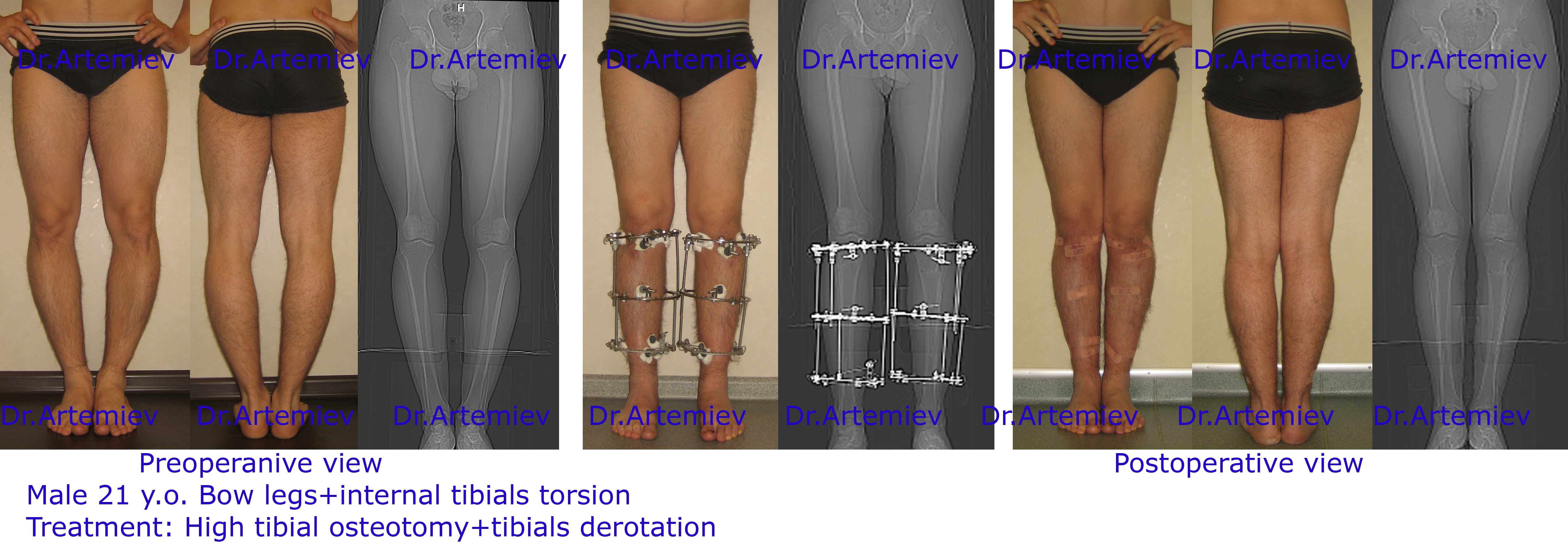
Bow Legs correction
Bow legs (varus knee deformity) - most common reason for surgical correction.
-
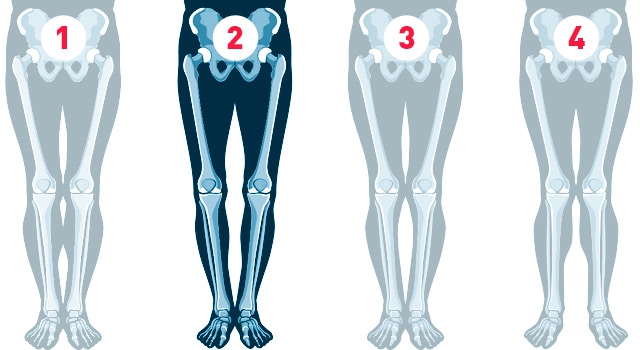 Ideal legs Bow legs False curvature Knock knees
Ideal legs Bow legs False curvature Knock knees
Main causes of bow legs (genu varum):
- Idiopatic genu varum;
- Knee osteoarthritis ;
- Posttraumatic deformity of femur or tibia;
- Diseases (Blount's disease, rachitis, etc.)
What is bow legs?
You can easily define your leg shape according to classification by yourself and consider if you need to change something or not.
- Ideal legs. Knees, calves and ankles are touching, three intervals between them.
- True O-shaped curvature (bow legs). Knees can't be attached to each other when ankles are touching. The main reason - varus deformity of the tibia below the knee.
- False curvature. It is in unique structure of soft tissues on the shin.
- True X-shaped curvature (knock knees) – knees are touching, ankles are separate. The main reason - valgus deformity of the femur or the tibia.
The aim of all reconstruction procedures is to restore normal mechanical axis of lower extremity. Surgery has certain challenges such as osteotomy level selection and extent of deformity correction wich depend on etiologe of varus deformation. It's very important that modern correction of shin deformation allows not only achieve pleasing aesthatic result but to prevent progress of joint diseas of knees in mature at late adulthood. Wrong load distribution in case of varus deformity causes premature "wear" of knee joints.
That is the reason why opportune correction of bow leg is the method of osteoarthrosis of a knee joint preventive measures.
Idiopatic bow legs
In younger patients bow legs deformity has spontaneous origin and represents congenital individual characteristic of the sceleton development which is inherited. Lower limb shape variations are related to age, sex and ethnicity. Genu varum is more prevalent in natives of Asian region (China, Japan, Korea) but can also occur worldwide. The main manifestation of bow legs deformity is a visible distance between the knees ina standing position with feet together. Anterior-posterior X-ray shows deviation of mechanical axis which is also called weight bearing line. Bilatreral limb deformation is usually found. Men and women seek help from an orthopaedic surgeon with equal frequency.
Knee osteoarthritis
Osteoarthritis is the most common joint disease. It is chracterized by joint pain and disfunction and, in advanced stages, joint contractures, muscle atrophy and limb deformity. Knee joint is one of the large joints which is affected most commonly. Understanding of early changes in the osteoarthritis progression is important, since these changes could still be reversible. Therefore, preventive treatment could be initiated to limit or reverse further progression of the disease. This is particularly true in young patients. High tibial osteotomy is an efficient method to treat unicondylar osteoarthritis. The rationale of high tibial osteotomy is to delay or prevent early degenerative changes by restoring a more favorable biomechanics. Thereby local compartmental overload is reduced by malalignment correction.
Posttraumatic deformity of femur or tibia
Severe femoral and tibial fracrures are often result in malunion. Posttraumatic deformation ususally leads to true shortening of leg (legs length discrepancy). Regardless of initial injury severity and malalignment of the limb, the Ilizarov method is used to restore axis and length of the limb completely.
Disorders (Blount's disease, rachitis, etc.)
Blount 's disease is a growth disorder of the tibia that result in lower limb inward angulation, resembling a bowleg. It is also known as "tibia vara". Early onset deformity is addressed as soon as possible to prevent further progression and subsequent joint deterioration.
Principles of leg shape correction by Ilizarov apparatus
Common principal of leg shape correction - osteotomy of the tibia in deformed area and fusion in correct position. It's not necessary to make an extensive approach to perform an osteotomy. Small stab incision (5-10 mm) is usualle appropriate. If shin soft tissues are aesthetically propitious an exellent result can be achieved without entire bone dissection but only by fissuring it from one side. After performing the oasteotomy the axis of extremity is adjusted for its correct layout and fixed in that position for further bone union.
Knock knees (valgus deformity) is corrected the same way, but direction of bone fragment displacement is the opposite.
A perfect device for limb axis correction and fixation is Ilizarov apparatus. Unfortunately not everyone can see advantages of this method. Largest experience of Ilizarov's apparatus application is acquired in Russia. Our experience in application of this method is more than 30 years and more than 4 thousand surgical operations in various different pathologies - leg length discrepancy, fractures malunions, as well as short stature and cosmetic correction of leg shape.
Ilizarov technique allows you to:
- correct malalignment;
- perform medialisation of bone fragments;
- eliminate rotational displacement;
- address protruding head of the fibula;
- lengthen the limb.
The Ilizarov apparatus can be closed with trouses without any problems and it weighs only 900 grams.
Ways to reduce the time of treatment and rehabilitation.
The average time from surgery up to the moment of removing the device is 3 months. In case of extension of the lower leg about 1 month should be added for each centimeter of lengthening. This term implies a gradual increase in loads and activity in the process of fixing and the ability to fully load the legs and walk freely without restrictions immediately after the removal of the devices. You can remove the devices before, for example after 50-60 days. However, it is then necessery to drastically reduse the load (up to walk with crutches) even during the last 45 days before the final seam.
Reducing the time of treatment can be processed as follows:
- a gradual increase in load on the legs (under medical supervision) shortens fixation by Ilizarov from 5 to 10%;
- incomplete osteotomy shortens fixing from 5 to 15%.
Features of rehabilitation
Rehabilitation functions as a limited recovey time - after surgery, the restoration of motor activity should take place gradually and in strict accordance with the doctor's recommendation. The gradual expansion of activity is facilitated by the use of special means of support and movement.

Modern means of support and movement after surgery

The Ilizarov apparatus is easily concealed under clothing and provides full function

The main factors that conributed to early rehabilitation, is self-discipline and motivation, as well as strict compliance to doctor's recommendation
Gallery